
How is Impingement and Rotator Cuff Tears Treated
Steve A. Mora, MD
Orange County Shoulder Specialist
Introduction
The term “Rotator Cuff” is used to describe the group of shoulder muscles and their tendons that helps control shoulder joint motion. The supraspinatus is at the top (superior) of the shoulder, the subscapularis is anterior (front), and the infraspinatus and teres minor are posterior (behind). These muscles insert or attach to the humeral head by way of their tendons. The tendons fuse together giving rise to the term “cuff.” Although each muscle acting alone may produce an isolated rotational movement of the shoulder, the role they play together is to help keep the humeral head (ball) centered within the glenoid (socket) as the powerful deltoid and other larger shoulder muscles act to lift the arm overhead.
Above the rotator cuff is a bony projection from the scapula (shoulder blade) called the acromion. The acromion forms the “ceiling” of the shoulder, serves as the point of origin for the deltoid muscle, and joins the clavicle (collarbone) to form the acromioclavicular (a/c) joint. Between the rotator cuff tendons and the acromion is a protective fluid-filled sack called a “bursa”. With normal humeral elevation there is some contact between the rotator cuff, the bursa, and the acromion. A healthy and strong rotator cuff holds the humeral head down in the socket and minimizes the upward pressure on the acromion.
Pathology
Rotator cuff pathology can be caused by extrinsic (outside) or intrinsic (from within) causes. Extrinsic examples include a traumatic tear in the tendon(s) from a fall or accident. Overuse injuries from repetitive lifting, pushing, pulling, or throwing are also extrinsic in nature. Intrinsic factors include poor blood supply, normal attrition or degeneration with aging, and calcific invasion of the tendon(s). Complete ruptures can also be seen acutely after a shoulder dislocation or from an acute forceful trauma. In cases of acute avulsions following a trauma the patient typically cannot raise the arm (drop arm sign).
Rotator cuff “tendonitis” is the term used to describe irritation of the tendon(s) either from excessive pressure on the acromion or less commonly from intrinsic tendon pathology. Irritation of the adjacent bursa is known as subdeltoid or subacromial “bursitis.” Repetitive overhead activities resulting in irritation of the tendon(s) and bursa from repeated contact with the undersurface of the acromion is called “Impingement Syndrome.”
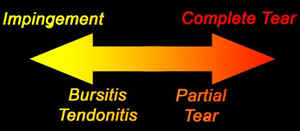
Rotator cuff dysfunction is typically a continuum of pathology ranging from tendonitis and bursitis on one end of the spectrum to partial tearing, to a complete tear in one or more of the tendons on the other extreme end. It is sometimes impossible to determine if the pain is due to tendinitis vs a tear. The presentation is very similar. Although the earlier stages may resolve with conservative care, actual tearing of the tendon can be more problematic. Because this area has a relatively poor blood supply, injury to the tendon here is very unlikely to actually heal. Additionally, the constant resting tension in the muscle-tendon unit, or “muscle tone”, pulls any detached fibers away from the bone, preventing their reattachment. Finally, joint fluid from within the shoulder may seep into the tear gap preventing the normal healing processes from occurring.

This diagram shows a typical rotator cuff tear involving the supraspinatus. The fact of the matter is that not all tears need surgery and not all tears increase in size. Sometimes a tear causes minimal pain and do not worsen with time. The bigger the tear, the more likely it will need surgery. Patients with rotator cuff pathology commonly present with an activity related dull ache in their upper lateral (outer) arm and shoulder. Above shoulder level activity is usually most difficult. Many people have little to no discomfort with below shoulder level activities such as golf, bowling, gardening, writing or typing, etc. Conversely, tennis, baseball/softball, basketball, swimming, painting, etc. will be more problematic.
Diagnosis
The diagnosis can usually be made with a good history, exam and plain X-Rays.
Typical pain patterns of shoulder problems:
-Pain around the deltoid area radiating anteriorly and laterally towards midarm is probably a impingement problem.
-Shoulder pain that is mostly anteriorly radiating to the biceps area is usually biceps tenditinis or a subscapularis tear.
-Shoulder pain on top of the shoulder radiating to clavicle, base of the neck and ear is probably due to AC Joint degeneration.
-Pain and catching with arm rotation might be a labral tear.
-Severe stiffness to the point that the arm seems locked is probably capsulitis or late effects of a rotator cuff tear.
-Excruciating pain that came on from one day to the next could be calcific tendinitis or adhesive capsulitis.
In addition pain at night or pain that wakes up the patient is very common. Pain reaching up or behind the body is common. In addition difficulty lifting items such as a gallon of milk can be a late sign of a tear.
X-rays will not show the rotator cuff, but they will reveal any evidence of arthritis, spurs within the shoulder, loose bodies, fractures from a related fall, abnormal displacement of the humerus out of the glenoid, calcific nodules, and congenital (birth) related problems. They can also show signs of massive chronic tears. Therefore, good quality x-rays are a must in the proper evaluation of the shoulder.

Magnetic Resonance Imaging or MRI has allowed visualization of the soft tissues of the body, including the rotator cuff. An MRI can depict tendonitis, partial tearing, and complete tears of the rotator cuff. While an MRI is not always necessary to diagnose a torn rotator cuff, it can be very helpful to determine which tendons are torn, how large the tear is, the degree of tendon retraction, the extent of muscle belly atrophy (shrinkage), and any coexisting problems. In order to identify small tears, contrast injected into the joint (arthrogram) may be necessary. Contrast injected into the veins prior to the MRI is not helpful.

Conservative Treatment
Can a rotator cuff tear be treated without surgery? The good news is that sometimes they can. Stretching is the main stay of physical therapy treatment. A tight shoulder is a painful shoulder. I helped to create shoulder stretching videos to help patients with stiffness. You can find these videos at www.MoraStretches.com. The focus of the stretching is to regain full passive motion equal to the opposite side. Posterior joint capsule can help the tendency of the humeral head to migrate superiorly toward the acromion with forward elevation. Manual soft tissue release (ART) around the scapula and chest wall can help to reduce the force across the joint and position the scapula in a optimized position.
Patients who fail to improve with initial conservative therapy, there may be a role for a corticosteroid (“cortisone”) injection.. The mechanism of how this technique may be helpful is not completely clear, but it may reduce bursal and tendon irritation and swelling. The cortisone does not just “mask” the problem, but helps break the cycle of pain, swelling, weakness, and continued impingement. Injection therapy may then help reduce pain and impingement and allow the individual to continue to work on rotator cuff strengthening. Current recommendations are that a maximum of 3 cortisone injections should be used per shoulder. There is some evidence in laboratory research that more than 3 cortisone injections around an otherwise healthy tendon may result in considerable weakening of the tendon and even rupture.
There are also some novel and or investigational treatments such as platelet rich plasma and adult stem cell treatment. I have used both of treatments and have had a modest level of success. I have seen best results in patients with partial tears.
Surgical Treatment
If a rotator cuff tear is large and or painful surgery can help.
If the patient feels that his or her quality of life is being significantly impacted by the shoulder dysfunction, then consideration of surgical intervention is certainly reasonable. Non operative treatment is usually done first however this is not the case for all situation. Patients with acute avulsions after a dislocation or fall do better if operated on early.
Patients with partial tears may also benefit from arthroscopic removal of spurs and shaving of loose torn fibers. If the partial tear is significant the surgeon may elect to repair the torn portion back to bone. Often times the shoulder has compensated and other co pathology exists along with the torn rotator cuff. For example the AC Joint may have developed degeneration, the capsule may have fibrosed, the biceps tendon may have become inflammed or torn, or the labrum may have become frayed. All of the pain causing pathology needs to be addressed at the time of the repair.
Rotator cuff repair is usually done arthroscopically (small incisions), under general anesthesia with a nerve block, in a outpatient surgery center. Strong stitches are placed in the torn ends of the rotator cuff tendons, and they are attached back the bone of the humerus through specially created tunnels or commercially available suture anchors. I have had great success suturing the tear down using a technique called “suture bridge” You can see a video about this if you click on : Suture Bridge Technique for Rotator Cuff Repair.
Surgery may not be as helpful for massive tears that have been present for many years. These tears often times cannot be pulled back to the bone. In these situations augmentation with various grafts might be helpful. Alternatively a reconstructive procedure called superior capsular reconstruction might be helpful. For more information about the superior capsular reconstruction you can visit this link: Superior Capsular Reconstruction for massive rotator cuff tears


Actual Case

Post Operative Rehabilitation
Whether done open or arthroscopically, rotator cuff repair is a major operation that requires considerable rehabilitation. The shoulder is typically protected in a sling for 6 weeks, although some gentle passive motion is typically begun almost immediately. The key during this period is to protect the repair tendon while at same time maintaining joint motion. Your surgeon may want you to start physical therapy 1-2 weeks after surgery or in cases of massive tears therapy may not be started until the surgeon feels it is safe to move the shoulder.
It takes 12 weeks for the tendon heal down to the bone. The attachment continues to mature and strengthen for 2 years. Despite the prolonged healing course, patients can very often begin light computer work in the sling 1 to 2 weeks, lift the arm overhead 2-3 months after surgery, participate in golf, fishing, and other less strenuous activities at 4 months, and return to full sports and work participation at 6-9+ months. It is not uncommon for patients to say that it took a whole year to feel near normal.
Long term studies have revealed 80 to 95 percent good to excellent results for rotator cuff repair done open or arthroscopically. Patient satisfaction rates are just as high. In the majority of these studies, over 90% of patients agreed that in respect they would have the surgery again if needed. Unfortunately patients with worker’s compensation cases or other litigation related to the shoulder injury have not enjoyed the same success rates. Good to excellent results in these patients may be as low as 65 to 75 percent, yet they are just as likely to indicate that they would have the surgery again if necessary. A well-motivated patient combined with a well-done repair and a comprehensive rehabilitation program, typically results in a satisfied patient who is able to return to his or her normal activities of daily living with little to no compromise.
I hope this information was helpful. Please contact me for any questions.
About Steve A. Mora MD:

Dr. Mora is a native of Orange County. He graduated from Anaheim High School in Orange County CA. He completed his training at the UC Irvine where he finished in the top of his class earning the coveted AOA Medical Society honors. He completed his Orthopedic Surgery training USC where he was elected chief resident of his class. He completed an extra year of training with a Sports Medicine, Cartilage, Shoulder, Hip arthroscopy and Knee Fellowship at Santa Monica Orthopaedic and Sports Medical Group. He is currently practicing Orthopedic Surgery in Orange County at Restore Orthopedics and Spine Center.
Dr. Mora’s practice focus on Sports Trauma, Knee Arthroscopy, Shoulder Arthroscopy, Hip Arthroscopy, Elbow Arthroscopy, and Cartilage Restoration of the knee. He sees athletes of all levels including professional soccer players and UFC/MMA combat athletes.
He is team doctor for the Anaheim Bolts pro indoor soccer team and Foothill High School.
Dr. Mora’s family heritage is Peruvian. He speaks fluent Spanish.
[embedyt] http://www.youtube.com/watch?v=NVlRGoxsuco[/embedyt]